Home Remedies
Natural Remedies for Restless Legs: Why They’re Worse at Night
The content on this website – including articles, event announcements, personal experiences, and recommendations – is for informational and educational purposes only and is not medical advice. Always consult a qualified healthcare professional before making any changes to your diet, exercise, supplements, sleep habits, or wellness routines, especially if you are pregnant, nursing, on medication, or have any medical condition.

It usually starts the same way. You’ve been in bed for twenty minutes, finally relaxed, and then — there it is. That deep, crawling, pulling sensation in your legs. Not quite pain, not quite an itch, but utterly impossible to ignore. The only thing that brings relief is moving, so you kick, stretch, walk to the kitchen and back, and start the whole miserable cycle over again.
If this is your nightly reality, you are dealing with Restless Legs Syndrome — also called Willis-Ekbom Disease — and you are far from alone. Estimates suggest between 7 and 10 percent of the population experiences RLS, making it one of the most underdiagnosed neurological conditions in the world. And because it primarily strikes at night, the sleep deprivation it creates ripples through every corner of daily life.
Here is what most articles about “home remedies for restless legs” completely fail to do: they hand you a list of generic tips — take a warm bath, try magnesium, cut the caffeine — without ever explaining why RLS happens at night in the first place, why some of the most common medications people take are silently making it dramatically worse, or what the right form and timing of magnesium supplementation actually looks like. This guide fills all of those gaps.
First, Let’s Settle What RLS Actually Is — Because Many People Confuse It

Before diving into remedies, it is worth spending a moment on what RLS is and, just as importantly, what it is not — because misidentifying the condition leads to mismanaged treatment.
Restless Legs Syndrome (RLS) is defined by four core features that must all be present for a formal diagnosis. There is an urge to move the legs, usually accompanied by uncomfortable sensations. That urge begins or gets significantly worse during rest or inactivity. It is at least partially and temporarily relieved by movement such as walking or stretching. And the symptoms are worse in the evening and at night compared to earlier in the day. All four features together distinguish RLS from general leg cramps, muscle twitching, positional discomfort, or simple restlessness from anxiety.
Periodic Limb Movement Disorder (PLMD) is a related but distinct condition that is frequently confused with RLS. In PLMD, the legs move involuntarily during sleep — repetitive kicks or jerks that happen every 20–40 seconds — but the person is often unaware of them. Their bed partner typically notices first. Unlike RLS, PLMD is not accompanied by the conscious urge to move and does not cause the pre-sleep crawling sensations. Some people have both conditions simultaneously. PLMD requires different management and is typically diagnosed via sleep study.
The Neuroscience Behind Why RLS Strikes at Night (Most Articles Never Explain This)
Understanding why RLS follows a strict circadian pattern is not just academically interesting — it directly informs the most effective timing strategies for every home remedy in this guide.
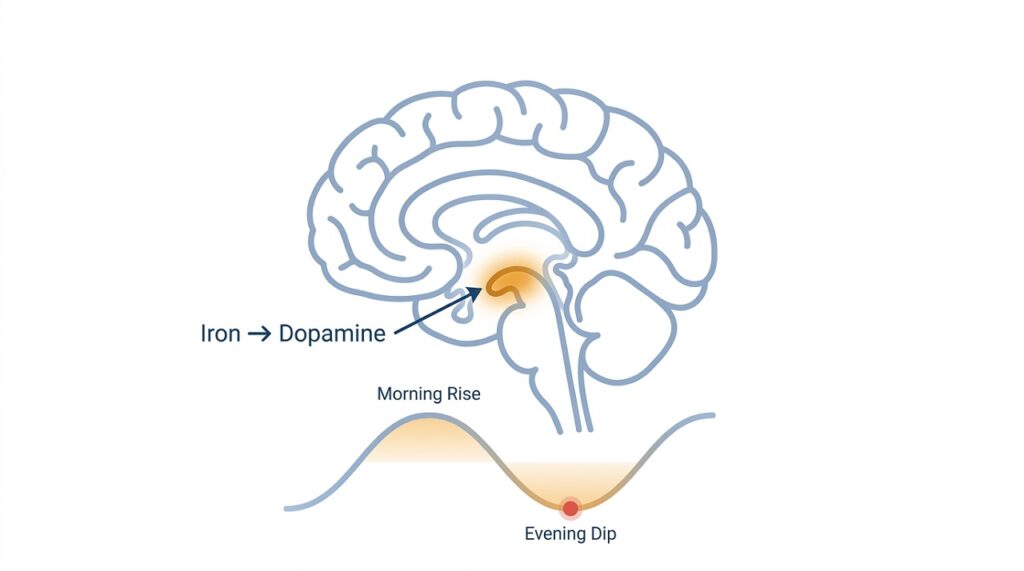
At the centre of RLS is a disruption in the dopamine pathway deep in the brain, specifically in a region called the substantia nigra and the basal ganglia — the same dopamine circuits involved in Parkinson’s disease, though through a different mechanism. Dopamine is responsible for coordinating smooth, controlled movement and suppressing unwanted nerve signals to the limbs. When dopamine signalling is disrupted, the brain essentially loses its ability to tell the legs to stay still.
Here is where iron enters the picture, and it is crucial. Iron is not just a blood mineral — it is a critical raw material for the production of tyrosine hydroxylase, the rate-limiting enzyme in dopamine synthesis. Studies using cerebrospinal fluid analysis, neuroimaging, and postmortem brain tissue have consistently found that RLS patients have reduced iron availability in specific brain regions — even when their blood iron levels appear perfectly normal. This brain-level iron insufficiency impairs dopamine regulation, and the result is the restless legs you experience every night.
Now for the circadian piece. Dopamine levels in the brain naturally follow a daily rhythm — they are highest in the afternoon and drop significantly in the evening. For most people this drop is inconsequential. But for someone whose dopamine system is already compromised by reduced brain iron, that evening drop pushes dopamine below the threshold needed to suppress the abnormal sensations — and RLS symptoms emerge or escalate. This is why your legs are almost always worse at night, and why strategies that support dopamine function or that are timed to the evening window provide the most relief.
The Hidden Trigger Hiding in Your Medicine Cabinet

This is the section that almost no home remedy article about RLS includes, and it is arguably the most important information here for a significant number of sufferers.
A wide range of commonly used medications — including several that are taken specifically to help with sleep — actually worsen RLS symptoms significantly by blocking dopamine receptors or otherwise disrupting the dopamine pathway your legs depend on.
Sedating antihistamines are the biggest trap. Diphenhydramine (the active ingredient in most over-the-counter sleep aids like Benadryl, Nytol, and Sominex) blocks H1 histamine receptors in a way that also antagonises dopamine receptors. Many RLS sufferers, frustrated by sleeplessness, reach for an OTC sleep aid — and make their RLS dramatically worse. If you are taking any antihistamine-based sleep product and your restless legs are severe, this may be the first thing to address.
Common cold and flu remedies containing antihistamines — including Night Nurse, Actifed, and many combination cold tablets — carry the same risk. Always read the active ingredients before taking any over-the-counter product if you have RLS.
Antidepressants are a complex and important category. SSRIs (selective serotonin reuptake inhibitors) and SNRIs (serotonin-norepinephrine reuptake inhibitors) — including fluoxetine, sertraline, citalopram, venlafaxine, and duloxetine — have all been documented to worsen RLS in clinical literature. A major 2024 pharmacovigilance study published in PMC analysing FDA adverse event data confirmed antidepressants as the most commonly reported drug category associated with drug-induced RLS. Mirtazapine (Zispin/Remeron) appears particularly problematic for RLS. The antidepressant least likely to worsen RLS is bupropion (Wellbutrin), which works through a dopaminergic rather than serotonergic mechanism — something worth discussing with your doctor if you need both depression and RLS management.
Proton pump inhibitors (PPIs) used for acid reflux — omeprazole, lansoprazole, pantoprazole — are flagged repeatedly in RLS patient communities and by RLS-UK as worsening symptoms, likely because long-term PPI use impairs iron absorption at the gut level, compounding the brain iron deficit at the core of RLS.
Anti-nausea medications including metoclopramide and prochlorperazine are potent dopamine antagonists and can trigger severe RLS flares. This is particularly important to flag before any surgical procedure where anti-nausea drugs are routinely administered.
This is not a reason to stop any prescribed medication without speaking to your doctor. It is a reason to have an informed conversation about whether a medication you are currently taking may be contributing to your RLS — and whether alternatives exist. If your RLS worsened around the time you started a new medication, this connection is worth investigating.
Natural Home Remedies That Have Genuine Evidence Behind Them
Magnesium Supplementation — The Form Matters Enormously

Magnesium is the most clinically investigated natural supplement for RLS, and the evidence has meaningfully strengthened in recent years. A 2022 randomised controlled trial published in BMC Complementary Medicine and Therapies found that magnesium oxide combined with vitamin B6 significantly improved both RLS symptom severity and sleep quality compared to placebo over two months. A 2024 pilot study published in the Journal of Clinical Sleep Medicine found that 200mg of magnesium citrate taken nightly for eight weeks produced significant reductions in validated RLS symptom scores.
Mechanistically, magnesium acts as a natural calcium channel blocker at nerve terminals — when magnesium levels are adequate, calcium’s ability to over-activate nerve signals is suppressed, reducing the abnormal sensory signals that manifest as restless legs. Magnesium also modulates NMDA receptors and supports dopamine signalling — directly relevant to RLS pathophysiology.
Why the form of magnesium you take matters: Magnesium oxide has the highest elemental magnesium content by weight but the lowest absorption rate — only around 4% is absorbed. Magnesium glycinate (magnesium bound to the amino acid glycine) and magnesium citrate have substantially better bioavailability, particularly for neurological applications. Glycinate is additionally well tolerated by the gut and less likely to cause the diarrhoea that high-dose oxide can produce. For RLS specifically, magnesium glycinate or citrate are the clinically rational choices over oxide.
Timing and dose: Take 200–400mg of elemental magnesium (glycinate or citrate) one to two hours before bed. This aligns the peak absorption window with the evening circadian drop in dopamine when RLS symptoms typically peak. Do not exceed 350mg supplemental magnesium daily without medical supervision, and consult a doctor before supplementing if you have kidney disease, as impaired kidneys cannot clear excess magnesium safely.
Iron — But Only If You Know Your Ferritin Number

Iron supplementation is one of the most biologically rational interventions for RLS given the iron-brain-dopamine pathway, but the way it is covered in virtually every online article is dangerously vague. “Get your iron checked” is not useful advice without context.
The number that matters for RLS is not your haemoglobin level — it is your serum ferritin level. Ferritin is the storage form of iron, and brain iron availability correlates with ferritin much more closely than with standard haemoglobin or serum iron. The standard laboratory “normal” range for ferritin typically bottoms out at 12–15 ng/mL. But the threshold that RLS specialists and neurologists use is considerably higher. The Restless Legs Syndrome Foundation and multiple sleep medicine guidelines suggest that a serum ferritin below 75 ng/mL in an RLS patient warrants iron supplementation discussion with a doctor — and that symptoms often improve as ferritin is raised toward the 100–150 ng/mL range.
This means you can have ferritin at 30–40 ng/mL, be told your iron is “normal” by a standard lab report, and still be iron-insufficient relative to what your brain needs for optimal dopamine regulation.
From a dietary standpoint: Iron-rich foods that support ferritin levels include lean red meat, dark leafy greens (spinach, kale), lentils, fortified cereals, pumpkin seeds, and dark chocolate. Pair iron-rich plant foods with vitamin C to significantly improve non-haem iron absorption — a squeeze of lemon juice over lentils, for instance, or a glass of orange juice alongside a fortified breakfast.
Avoid iron supplementation without a blood test first. Iron overload is genuinely harmful, particularly for men and post-menopausal women whose bodies don’t have a monthly route of iron excretion. Self-supplementing iron without knowing your baseline ferritin is not a safe approach.
Leg Massage — The First-Line Remedy That a Sleep Neurologist Actually Recommends
Dr J. Andrew Berkowski, a sleep neurologist quoted by Cleveland Clinic, describes leg massage as his first-line recommendation before considering any medication for RLS. This is not a platitude — there is a mechanism behind it. Manual stimulation of the legs activates large-fibre sensory neurons that compete with and partially suppress the small-fibre abnormal nerve signals responsible for RLS discomfort, through a mechanism similar to the gate control theory of pain.
How to do it effectively: Sit on the edge of the bed or floor. Using both hands, apply firm upward strokes from the ankle toward the knee, then use circular thumb pressure along the calf muscles and the back of the knee. Spend 5–10 minutes per leg. For enhanced effect, warm a small amount of coconut oil or arnica massage oil between your palms first — warmth amplifies the circulatory benefits and the massage becomes more pleasurable, making consistency more likely.
Consistency matters more than technique here. A brief daily evening massage, performed 30–60 minutes before bed as part of a pre-sleep wind-down routine, is more effective than an occasional longer session.
Temperature Therapy — Hot, Cold, or Both?
Almost every article on RLS mentions “warm bath” and leaves it there. The reality is more nuanced, and knowing which temperature to use and when can meaningfully change the outcome.
Heat (warm bath, heated compress, or electric blanket on low) works by dilating blood vessels and improving circulation to the legs, relaxing muscle tension, and promoting the parasympathetic “rest and digest” nervous system state that counters the hyperexcitability underlying RLS. A warm bath taken 60–90 minutes before bed also produces a temporary core body temperature rise followed by a drop — and that temperature drop is a powerful sleep-onset trigger. For most RLS sufferers, heat is the right choice as part of a bedtime routine.
Cold (ice pack, cold compress, or cool water immersion for the feet and calves) works differently — it reduces nerve conduction velocity, essentially “numbing down” the overactive sensory signals temporarily. Some RLS sufferers find cold more effective than heat, particularly for the crawling sensations rather than the muscle tension component. The only way to know which works better for you is to experiment systematically.
Contrast therapy — alternating between warm and cold application — is used by some RLS patients with good results. Spend 3 minutes with a warm compress on both calves, then 1 minute with a cold compress, and repeat the cycle three times. The alternating vasodilation and vasoconstriction creates a pumping effect in the peripheral circulation, which can clear metabolic waste from muscle tissue and reduce the neurological irritability that drives RLS.
Exercise — The Critical Timing Window Nobody Tells You About
Regular moderate exercise reduces RLS severity over time — this is well-supported in the literature. But the timing and intensity relationship with RLS is a paradox that most articles completely ignore, and getting it wrong can make a bad night dramatically worse.
What helps: Moderate aerobic exercise performed in the late afternoon — a 30-minute walk, a gentle cycle, light swimming — consistently reduces RLS symptom severity when done regularly. The mechanism involves improved dopamine receptor sensitivity, better peripheral circulation, and reduction in the chronic low-grade inflammation that aggravates neural excitability.
What makes it worse: Vigorous exercise — intense gym sessions, long runs, heavy resistance training — particularly when performed within 3–4 hours of bedtime, can significantly worsen RLS symptoms that night. This happens because intense exercise creates metabolic stress in muscle tissue, increases excitatory neurotransmitter activity, and elevates core body temperature in a way that disrupts the sleep-onset signals your body needs.
The practical rule: keep your exercise moderate, keep it consistent, and keep it finished by mid-evening at the latest. If you currently exercise intensely in the evening and your RLS is severe, shifting your workout to the morning or afternoon is worth trying before anything else.
The Pre-Sleep Routine: Timing and Environment

Because RLS is driven by a circadian mechanism — dopamine naturally falling in the evening — creating a pre-sleep environment that minimises triggers and supports dopamine function is not generic wellness advice. It is directly therapeutic.
Caffeine has a longer half-life than most people realise. The half-life of caffeine in the body is approximately 5–7 hours for most adults, meaning a 3pm coffee still has half of its caffeine active in your system at 8–10pm. Caffeine disrupts adenosine signalling in the brain — and adenosine dysfunction is a documented secondary mechanism in RLS pathophysiology, particularly in iron-deficient states. Cutting caffeine before noon is the right standard for RLS sufferers, not “avoid coffee after 6pm.”
Alcohol is a short-term relaxant that disrupts sleep architecture in the second half of the night and worsens RLS symptoms in many sufferers. It suppresses deep sleep stages, raises body temperature, and impairs the dopamine-serotonin balance in ways that typically amplify restless legs symptoms in the early hours of the morning.
Smoking worsens peripheral circulation, impairs iron absorption, and has been consistently identified as an RLS aggravator in epidemiological studies.
A consistent sleep and wake schedule supports the stability of your circadian rhythm — including the dopamine cycle. Going to bed and waking at erratic times destabilises this rhythm and creates the conditions for more frequent and more severe RLS episodes.
RLS During Pregnancy — A Separate Conversation
Pregnancy is one of the most common triggers of RLS, affecting an estimated 20–25% of pregnant women, typically worsening in the third trimester and usually resolving within weeks of delivery. The mechanism overlaps with general RLS — iron and folate deficiencies are extremely common in pregnancy — but management requires specific considerations.
Many of the natural approaches in this guide are pregnancy-safe: leg massage, moderate exercise, temperature therapy, dietary iron optimisation, and sleep scheduling. However, magnesium supplementation during pregnancy should be discussed with an obstetrician before starting, as magnesium interacts with several pregnancy-specific physiological processes.
Importantly, many pharmacological RLS treatments are contraindicated in pregnancy. This makes the natural approaches in this guide particularly relevant for pregnant women — but it also makes professional guidance even more important. If you are pregnant and experiencing significant RLS, raise it explicitly with your midwife or obstetrician rather than managing it entirely on your own.
When to See a Doctor — and What to Ask For

Home remedies are effective for mild-to-moderate RLS and for identifying and removing aggravating factors. But several presentations warrant professional evaluation without delay.
See a doctor if your RLS is severe enough to prevent sleep on most nights, if symptoms are affecting your daytime function, concentration, mood, or cardiovascular health, if you are pregnant and experiencing RLS, if you suspect a medication you are taking is worsening your symptoms, or if your legs are moving involuntarily during sleep (which may indicate PLMD rather than, or in addition to, RLS).
When you see your doctor, ask specifically for a serum ferritin test — not just a standard “iron” or haemoglobin test. Ask what your ferritin number is, and ask whether it is above the 75 ng/mL threshold relevant to RLS. This is the most commonly missed clinical step in general practice management of RLS, and advocating for it yourself can make a significant difference.
Frequently Asked Questions
Q: What is the fastest way to stop restless legs at night when they’re already bad?
The fastest-acting approaches are physical movement combined with temperature therapy. Get out of bed, walk for 5 minutes, then apply a warm or cold compress (whichever works better for you) to your calves for 10 minutes while seated. Follow this with a firm leg massage. This combination addresses the neurological irritability, improves circulation, and activates competing nerve fibres — giving you the best chance of being able to get back to sleep within 20–30 minutes.
Q: Does magnesium really help restless legs?
The evidence has strengthened considerably. A 2022 RCT and a 2024 pilot study both found meaningful symptom improvement. A 2024 systematic review of 10 trials found magnesium oxide and B6 significantly improved sleep quality and RLS symptoms. The key is choosing the right form (glycinate or citrate, not oxide alone) and taking it in the evening at an appropriate dose. It is most effective in people with documented or subclinical magnesium deficiency.
Q: Can stretching alone control RLS symptoms?
Stretching alone is rarely sufficient for moderate-to-severe RLS, but targeted stretching of the calves, hamstrings, and hip flexors performed consistently before bed can meaningfully reduce symptom onset in milder cases. Yoga specifically has been studied for RLS — a small trial found that a consistent yoga practice reduced both symptom severity and psychological distress associated with RLS. Think of stretching as a valuable component of a broader evening routine rather than a standalone solution.
Q: Is RLS a lifelong condition?
For primary (idiopathic) RLS with a genetic component, it is typically a chronic condition, though many people experience periods of remission. For secondary RLS caused by identifiable factors — iron deficiency, pregnancy, medication side effects — addressing the underlying cause can resolve symptoms entirely. This distinction matters enormously, which is why identifying and correcting secondary causes (including the medication triggers discussed above) should always be the first step.
Q: Can diet alone control restless legs?
Diet can play a meaningful supportive role, particularly through optimising iron, magnesium, folate, and vitamin C intake, and by eliminating known aggravators like alcohol and excessive caffeine. But for most people with established RLS, dietary changes alone are insufficient — they work best as part of a comprehensive approach that includes the timing, temperature, movement, and supplementation strategies covered in this guide.
Q: Does RLS get worse with age?
Generally yes — symptom frequency and severity tend to increase with age in primary RLS, partly because iron metabolism and dopamine receptor sensitivity both change with ageing. However, this is not inevitable, and adopting the management strategies in this guide consistently can significantly slow or limit that progression. Identifying and correcting any secondary contributing factors, particularly iron status and medication interactions, becomes increasingly important with age.
Scientific References
- Allen RP, et al. (2013). Restless legs syndrome/Willis-Ekbom disease diagnostic criteria: updated International Restless Legs Syndrome Study Group (IRLSSG) consensus criteria. Sleep Medicine. https://doi.org/10.1016/j.sleep.2012.10.011
- Earley CJ, Connor JR, et al. (2014). Altered brain iron homeostasis and dopaminergic function in Restless Legs Syndrome (Willis-Ekbom Disease). JAMA Neurology. https://pubmed.ncbi.nlm.nih.gov/25201131/
- Jadidi A, et al. (2022). Therapeutic effects of magnesium and vitamin B6 in alleviating the symptoms of restless legs syndrome: a randomized controlled clinical trial. BMC Complementary Medicine and Therapies. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9804944/
- Gorantla S, et al. (2024). Magnesium citrate monotherapy improves restless legs syndrome symptoms and multiple suggested immobilization test scores: an open-label pilot study. Journal of Clinical Sleep Medicine. https://doi.org/10.5664/jcsm.11264
- González-Parejo P, et al. (2024). Effects of Dietary Supplementation in Patients with Restless Legs Syndrome: A Systematic Review. Nutrients. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11280425/
- Guo S, et al. (2017). Iron, dopamine, genetics, and hormones in the pathophysiology of restless legs syndrome. Journal of Neurology. https://doi.org/10.1007/s00415-017-8431-1
- Xie M, et al. (2023). Circadian rhythm in restless legs syndrome. Frontiers in Neurology. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9995399/
- Salas RE, et al. (2014). Medications Associated with Restless Legs Syndrome: A Case Control Study. Journal of Clinical Sleep Medicine. https://pmc.ncbi.nlm.nih.gov/articles/PMC4172448/
- Hua Y, et al. (2025). Exploring the Top 50 Drugs Associated with Restless Legs Syndrome Based on FDA Data 2004–2024. PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC12087588/
- Winkelman JW, et al. (2016). The Neurobiology and Treatment of Restless Legs Syndrome. Biological Psychiatry. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5214985/
- Restless Legs Syndrome Foundation. Serum Ferritin and RLS. https://www.rls.org/understanding-rls/medical-information
This article is for informational purposes only and does not constitute medical advice. Restless Legs Syndrome can be associated with underlying medical conditions and medication interactions that require professional evaluation. Please consult a qualified healthcare provider before starting any supplement regimen or making changes to prescribed medications.













Living with eczema can wear you down fast. The itching, dryness, and red patches can flare without warning, especially with atopic dermatitis, a common inflammatory skin condition. You want relief that feels safe, simple, and easy to use at home.
The best homemade remedies for eczema focus on deep moisture, gentle care, and calming inflamed skin using simple, natural ingredients you can use every day. These remedies support your skin barrier and help reduce irritation without harsh products. They work best when you use them with steady daily habits.

You can take control of this chronic skin condition by learning what soothes your skin and what triggers flare-ups. Small changes in how you care for your skin can ease discomfort and help you feel more comfortable in your own body.
Key Takeaways
- Eczema is a chronic inflammatory skin condition that needs gentle daily care.
- Homemade remedies help soothe skin by locking in moisture and reducing irritation.
- Simple habits can lower flare-ups and support long-term skin comfort.
Understanding Eczema and Its Symptoms

Eczema affects how your skin looks, feels, and protects you. It causes visible changes, ongoing discomfort, and repeated flare-ups tied to daily triggers and skin barrier damage.
What Is Eczema?
Eczema is a chronic skin condition that causes inflammation and irritation. Doctors often call the most common type atopic dermatitis. You can have symptoms for years, with periods of calm skin and sudden eczema flares.
This inflammatory skin condition is not contagious. It often starts in childhood but can appear at any age. Many people manage symptoms with daily care and home remedies, as explained by the Cleveland Clinic’s overview of eczema.
Your skin reacts more strongly to irritants, allergens, and stress. That reaction leads to redness, itching, and damage to the skin surface.
Typical Eczema Symptoms
Eczema symptoms vary, but most people notice a clear pattern. Itchy skin usually comes first and can feel intense, especially at night.
Common symptoms include:
| Symptom | What You Notice |
|---|---|
| Dry skin | Rough, flaky, or tight areas |
| Redness | Pink to deep red patches |
| Itching | Mild to severe urge to scratch |
| Thick skin | Skin hardens after repeated scratching |
Scratching may give short relief, but it often worsens irritation. Medical News Today explains how these symptoms develop and change over time in its guide to eczema symptoms and home treatment.
Eczema Flare-Ups and Triggers
An eczema flare-up happens when symptoms suddenly worsen. You may notice stronger itching, darker redness, or cracked skin within hours or days.
Common eczema flare triggers include:
- Dry air or cold weather
- Harsh soaps or fragrances
- Stress and poor sleep
- Sweating or rough fabrics
You may not react to every trigger. Keeping track of your eczema flare-ups helps you spot patterns. WebMD describes how everyday exposures can lead to flares in its article on eczema treatment at home.
The Role of the Skin Barrier
Your skin barrier acts like a shield that locks in moisture and blocks irritants. With eczema, this barrier does not work well.
When the barrier weakens, water escapes and dry skin forms. Irritants then enter more easily, which fuels inflammation and itching. This cycle drives repeated eczema flares.
Protecting the skin barrier is a core goal of care. Gentle cleansing, frequent moisturizing, and avoiding triggers all support barrier repair. Verywell Health explains how barrier care fits into daily routines in its review of home remedies for eczema.
Best Homemade Remedies for Eczema Relief
You can ease itching, dryness, and redness with simple items you may already have at home. These natural remedies focus on moisture, gentle cleansing, and skin barrier support to help calm eczema-prone skin.
Colloidal Oatmeal Baths and Pastes
Colloidal oatmeal comes from finely ground oats mixed into water. You can add it to a warm bath to soothe itching and soften dry skin. A colloidal oatmeal bath coats your skin and helps reduce irritation.
Dermatology groups often recommend this option for eczema relief because it works as a mild emollient. It also supports your skin barrier. The Cleveland Clinic explains how colloidal oatmeal baths help eczema symptoms.
How to use
- Add 1 cup of colloidal oatmeal to a warm bath
- Soak for 10–15 minutes
- Pat skin dry and apply moisturizer right away
For small areas, mix oatmeal with water to form a paste. Apply for 10 minutes, then rinse gently.
Virgin Coconut Oil and Cold-Pressed Coconut Oil
Coconut oil helps seal in moisture and reduce dryness. Virgin coconut oil and cold-pressed coconut oil work best because they contain fewer added chemicals.
This oil acts as a simple emollient. You can use it as part of your eczema home remedies routine, especially after bathing. WebMD notes that coconut oil can help moisturize eczema-prone skin.
Tips for safe use
- Choose unrefined, cold-pressed oil
- Apply a thin layer to damp skin
- Avoid use on broken or oozing skin
Stop use if you notice burning or increased redness.
Aloe Vera Gel
Aloe vera gel cools the skin and helps reduce irritation. Many people use it for itching linked to eczema flare-ups. The gel absorbs fast and does not leave a greasy feel.
Medical News Today describes how aloe vera gel may calm eczema-related inflammation. You can use pure aloe vera gel straight from the plant or a store product with few additives.
Best practices
- Use clear, fragrance-free gel
- Apply 1–2 times daily
- Test on a small patch first
Avoid products with alcohol, which can dry your skin.
Apple Cider Vinegar Baths and Compresses
Apple cider vinegar may help balance skin acidity. This can support your skin barrier when used with care. Many people try diluted apple cider vinegar as part of natural eczema treatment.
Health experts stress proper dilution to avoid burns. Greatist explains safe use of apple cider vinegar for eczema relief.
Safe dilution guide
| Use | Vinegar | Water |
|---|---|---|
| Bath | 1 cup | Full tub |
| Compress | 1 tbsp | 1 cup |
Never apply undiluted vinegar. Stop if stinging lasts more than a few seconds.
Hydration and Moisturizing Strategies

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Strong hydration habits and the right moisturizer choices reduce dryness, itching, and skin cracking. Simple ingredients and steady use matter more than expensive products or complex routines.
Choosing Effective Moisturizers
You get the best results from a fragrance-free moisturizer made for sensitive skin. Fragrances often trigger flares and add no benefit. Look for eczema creams that list ceramides, glycerin, or hyaluronic acid, since these support hydration and help repair the skin barrier.
Thick products work better than lotions. Ointments and creams seal in water longer, especially after bathing. Many dermatologists recommend simple options like petroleum jelly or Vaseline, which reduce moisture loss and limit irritation. WebMD explains why regular moisturizing plays a central role in eczema home treatment.
Apply moisturizer within three minutes of washing your skin. This timing helps trap water before it evaporates.
DIY Eczema Creams and Balms
You can control ingredients and avoid irritants with a homemade eczema cream. Simple recipes often rely on a small number of emollients that soothe dry skin. Healthline reviews how basic blends using plant-based fats can support homemade creams for eczema relief.
A basic balm may include:
- Shea butter for softness and moisture retention
- Olive oil for gentle skin conditioning
- A small amount of glycerin to attract water
Mix and store creams in a clean, sealed container. Test on a small patch of skin before regular use to reduce the risk of irritation.
Key Emollient Ingredients
Emollients smooth rough skin and reduce flaking by filling gaps between skin cells. They form the base of most eczema creams and balms.
Common options include:
| Ingredient | Why it helps |
|---|---|
| Shea butter | Softens skin and supports barrier repair |
| Petroleum jelly | Locks in moisture and prevents water loss |
| Olive oil | Adds light hydration for very dry areas |
| Glycerin | Pulls water into the outer skin layer |
Medical News Today notes that emollients and regular hydration are core parts of effective home treatment for eczema. Some people also tolerate niacinamide, which may calm redness when used in low amounts.
FAQ: Best Homemade Remedies for Eczema
What is eczema, and what causes it?
Eczema, or atopic dermatitis, is a chronic skin condition characterized by dry, itchy, and inflamed skin. It can be triggered by various factors, including allergens (like pollen or pet dander), irritants (such as soaps or detergents), stress, and changes in temperature or humidity. Genetics also play a significant role, as individuals with a family history of eczema or allergies are more prone to develop the condition.
What are some effective homemade remedies for eczema?
Several homemade remedies can help alleviate eczema symptoms, including:
Coconut Oil: Acts as a moisturizer and has anti-inflammatory properties.
Oatmeal Baths: Colloidal oatmeal can soothe irritated skin and reduce itching.
Aloe Vera: Known for its healing properties, it can help reduce inflammation and hydrate the skin.
Honey: Has natural antibacterial properties and can help keep the skin moisturized.
Shea Butter: Rich in fatty acids, it helps to moisturize and protect the skin barrier.
How do I use these homemade remedies?
Coconut Oil: Apply a thin layer to affected areas after bathing or whenever the skin feels dry.
Oatmeal Baths: Add 1-2 cups of colloidal oatmeal to a warm bath and soak for 15-20 minutes. Pat the skin dry gently afterward.
Aloe Vera: Apply pure aloe vera gel directly to the skin as needed for relief.
Honey: Use as a topical treatment on affected areas; leave on for 20-30 minutes before rinsing off.
Shea Butter: Massage into the skin, particularly after bathing, to lock in moisture.
Are there any side effects or risks associated with these remedies?
While homemade remedies are generally safe, some individuals may experience allergic reactions. It’s essential to perform a patch test before using any new ingredient. If irritation occurs, discontinue use immediately and consult a healthcare professional.
How long does it take to see results from these remedies?
Results can vary depending on the individual and the severity of the eczema. Many people notice improvements within a few days to weeks of consistent use. However, chronic eczema may require ongoing management and consultation with a healthcare provider for more comprehensive treatment.
Can these remedies be used alongside prescribed medications?
Yes, many homemade remedies can complement prescribed treatments. However, it’s crucial to consult with a healthcare professional before combining treatments to avoid potential interactions or complications.
What should I do if my eczema worsens despite using homemade remedies?
If your eczema worsens or does not improve after a few weeks of using homemade remedies, it’s important to consult a healthcare provider or dermatologist. They can provide a more tailored treatment plan and address any underlying issues.
Are there any lifestyle changes that can help manage eczema?
Yes, several lifestyle changes can help manage eczema, including:
Moisturizing regularly: Use emollients to keep the skin hydrated.
Avoiding triggers: Identify and minimize exposure to known irritants and allergens.
Wearing breathable fabrics: Opt for cotton and avoid wool or synthetic materials.
Managing stress: Practice relaxation techniques like yoga or meditation to help reduce flare-ups.
Where can I find more information or support for managing eczema?
For more detailed information and support, consider visiting reputable websites such as the National Eczema Association or consulting with a healthcare professional. Online support groups and forums can also provide community support and shared experiences.
Are there any costs associated with these homemade remedies?
The costs can vary based on the ingredients you choose to use. Many homemade remedies utilize common household items, making them relatively inexpensive. However, if you opt for organic or specialty products, prices may increase. Overall, homemade remedies tend to be more affordable than commercial treatments.
If you have further questions or need personalized advice, feel free to reach out to a healthcare professional or dermatologist.

Introduction
You’re doubled over with cramps… or constantly running to the bathroom… or so bloated you can’t button your jeans. These aren’t just passing annoyances—they’re signs your intestines are inflamed and crying out for relief.
Intestinal inflammation can stem from many causes—food poisoning, stress-induced IBS, IBD flares, or even gut dysbiosis—but that doesn’t mean one remedy fits all.
The problem with many online “natural remedy” lists is that they lump everyone together. But bloating and diarrhea aren’t treated the same way—and using the wrong home remedy (like strong ginger during an ulcerative colitis flare) can make things worse.
This guide aligns natural care with your specific symptom—bringing together remedies and safety insights directly from trusted health sources like Tuasaude, Rupa Health, and the Mayo Clinic.
⚠️ Disclaimer: These remedies are for mild, short-term symptoms only. According to Tuasaude, if you don’t notice improvement within 2 days or feel progressively worse, see a doctor. This content is for informational purposes and is not medical advice. Always consult your healthcare provider before trying new remedies—especially if you have IBD, are pregnant, or take medications.
How to Identify Your Dominant Symptom

Before reaching for herbs or teas, pause to identify what your body is actually saying. Each digestive symptom signals a different imbalance—and knowing which one dominates helps you choose the safest, most effective home care.
- Bloating + gas: Often linked to intestinal irritation or infection. Caution: Avoid hard-to-digest foods, as noted by Tuasaude during recovery.
- Cramping + pain: May result from intestinal wall inflammation or spasms (Tuasaude; Rupa Health).
- Watery diarrhea (no blood): Common in viral or bacterial intestinal infections (Tuasaude).
- Mucus in stool: Can occur with gut irritation; monitor closely and seek care if persistent.
- Nausea + appetite loss: Frequently seen in acute intestinal infections (Tuasaude).
🚨 Red flags (per Tuasaude and Mayo Clinic): Blood in stool, fever, dehydration, or symptoms lasting more than 2 days → seek urgent medical care.
Targeted Remedies by Symptom
The following remedies are drawn directly from Tuasaude’s home treatments for intestinal infections and Rupa Health’s guidance on herbs for intestinal inflammation.
For Bloating & Excess Gas

Goal: Relax intestinal smooth muscle, reduce fermentation, and expel trapped gas.
Peppermint Tea
- How it works: Peppermint soothes irritation of the intestinal walls and absorbs excess gas. It also has antispasmodic properties that relieve abdominal discomfort (Tuasaude). Rupa Health adds that peppermint oil (especially enteric-coated) relaxes gastrointestinal smooth muscle and is supported in IBS guidelines.
- Recipe: Steep 6 fresh peppermint leaves in 1 cup boiling water for 5–10 minutes. Strain and drink (Tuasaude).
- Frequency: Several times daily (Tuasaude).
- Caution: Not recommended if you have GERD or active IBD flares—consult your provider (Rupa Health).
Fennel Tea
- How it works: Fennel contains anethole and other compounds with antispasmodic, anti-inflammatory, and digestive properties that reduce cramping, gas, and nausea (Tuasaude; Rupa Health).
- Recipe: Add 1 tsp fennel seeds to 1 cup boiling water. Cover and steep 10–15 minutes. Strain (Tuasaude).
- Frequency: 2–3 cups per day (Tuasaude).
- Caution: Should not be used by pregnant or breastfeeding women (Tuasaude).
“For deeper insight into how these herbs work, explore our guide to evidence-based herbs for inflamed intestines“
For Cramping & Abdominal Pain

Goal: Calm spasms and soothe irritated intestinal lining.
Chamomile Tea
- How it works: Chamomile is rich in apigenin and other phenolic compounds that reduce gastrointestinal stimulation and relieve cramps (Tuasaude). Rupa Health notes it helps dispel trapped gas and relaxes intestinal smooth muscle.
- Recipe: Steep 2 tsp dried chamomile flowers in 250 mL boiling water for 5–10 minutes. Strain (Tuasaude).
- Frequency: Up to 3–4 times daily (Tuasaude; Rupa Health).
- Safety: Generally well-tolerated; avoid if allergic to ragweed.
Low-Dose Ginger Water
- How it works: Ginger root has antiviral and antibacterial properties that help eliminate intestinal pathogens. It also regulates intestinal flow and reduces inflammation of the lining, easing pain and swelling (Tuasaude). Rupa Health confirms ginger relaxes digestive muscles and eases spasms.
- Recipe: Blend 2 cm peeled, crushed ginger with a few drops of honey and 1 glass of water. Strain (Tuasaude).
- Frequency: At least 3 times daily during acute infection (Tuasaude).
- Caution: Avoid if you have bowel strictures or are on blood thinners (Rupa Health).
For Diarrhea (Non-Bloody)

Goal: Prevent dehydration and soothe irritated mucosa.
Homemade Electrolyte Solution
- Recipe: Mix 1 liter of boiled or bottled water with 1 heaping tbsp sugar and 1 tsp salt (Tuasaude).
- How it helps: Replenishes minerals and sugars lost through vomiting or diarrhea; prevents dehydration (Tuasaude).
- Frequency: Drink 2–3 liters per day in small sips (Tuasaude).
Aloe Vera (Inner Gel Only)
- How it works: The gel from inside aloe leaves contains polysaccharides that soothe irritated gastrointestinal tissues (Rupa Health).
- Dosage: Use only the inner fillet/gel—never aloe latex.
- ⚠️ Warning: Aloe latex has strong laxative effects and can worsen diarrhea or cause electrolyte imbalance (Rupa Health).
For Nausea & Loss of Appetite
Goal: Calm the stomach and stimulate gentle digestion.
Ginger-Honey Water
- Recipe: Blend crushed ginger with honey and water (Tuasaude).
- Frequency: At least 3x/day during infection (Tuasaude).
- Mechanism: Ginger combats nausea and regulates digestive flow (Tuasaude; Rupa Health).
Chamomile + Lemon Water
- Lemon water: Tuasaude recommends warm water with half a lemon daily in the morning to stimulate intestinal flow and relieve cramps, loss of appetite, and diarrhea.
- Caution: Lemon is acidic—skip if you have ulcers or mucosal sensitivity.
What NOT to Do Based on Your Symptom

Tuasaude and Mayo Clinic strongly advise against the following during intestinal inflammation:
- Avoid anti-diarrheal medications—they can trap pathogens and prolong infection (Tuasaude).
- Avoid NSAIDs like ibuprofen—they worsen intestinal inflammation and can aggravate IBD (Mayo Clinic).
- Avoid alcohol, soda, greasy foods, and hard-to-digest meals during recovery (Tuasaude).
- Do not interrupt prescribed treatment without medical guidance (Tuasaude).
When to Stop Home Remedies & Seek Help

Per Tuasaude and Mayo Clinic, stop home remedies and see a doctor if:
- Symptoms last more than 2 days
- You develop fever, blood in stool, black/tarry stools, or severe dehydration
- You have known IBD, strictures, or are immunocompromised
Mayo Clinic emphasizes that while diet and home care help manage symptoms, IBD requires ongoing medical supervision—especially to monitor cancer risk and medication needs.
“If you’re unsure whether your symptoms are serious, review our full checklist on when to see a doctor for inflamed intestines.”
Frequently Asked Questions (FAQ)
Q: Can I use peppermint oil capsules instead of tea?
A: Rupa Health notes that enteric-coated peppermint oil is used in clinical settings for IBS. However, during active intestinal inflammation or infection, Tuasaude recommends tea only. Always consult your doctor first.
Q: Is lemon water safe during intestinal inflammation?
A: Tuasaude includes lemon water as a remedy for intestinal infections. However, if you have ulcers, severe mucosal damage, or IBD flares, acidic drinks may irritate—use cautiously.
Q: How long should I try one remedy before switching?
A: Tuasaude advises: If no improvement in 2 days, seek medical care. Do not self-treat beyond this window.
Q: Are these remedies safe for IBD patients?
A: Not during active flares. Mayo Clinic states that IBD management requires medical therapy. Rupa Health adds that herbs like slippery elm or chamomile may support remission—but only under provider guidance.
“For a detailed safety guide, see our post on safe herbal remedies for IBD patients.”
📖 Want the full picture?
Explore our Ultimate Guide to Home Remedies for Inflamed Intestines—a complete, free resource that ties together symptom relief, herb safety, recovery plans, and red flags in one place.
Sources Used (Direct Attribution)
- Tuasaude. (2024). Home Remedies for Intestinal Infections. https://www.tuasaude.com/en/home-remedies-for-intestinal-infections/
→ Provides all core remedies: ginger water, peppermint tea, fennel, chamomile, lemon water, electrolyte solution, garlic tea, and recovery guidelines. - Rupa Health. (2024). Top 10 Herbs for Intestinal Inflammation. https://www.rupahealth.com/post/top-10-herbs-for-intestinal-inflammation
→ Details mechanisms of peppermint, ginger, chamomile, aloe vera, fennel, and safety cautions (e.g., aloe latex, DGL licorice). - Mayo Clinic. (2024). Inflammatory Bowel Disease: Diagnosis and Treatment. https://www.mayoclinic.org/diseases-conditions/inflammatory-bowel-disease/diagnosis-treatment/drc-20353320
→ Advises against NSAIDs, emphasizes medical care for IBD, and outlines when to seek help. - Medical News Today. (2024). Foods That Heal Colon Inflammation. https://www.medicalnewstoday.com/articles/foods-that-heal-colon-inflammation
→ Supports gentle reintroduction of fiber, hydration, and whole foods post-flare (used contextually for recovery phase). - Gaucher Disease Blog. (2024). 4 Ways to Improve Gut Health Naturally. https://www.gaucherdisease.org/blog/4-ways-to-improve-gut-health-naturally/
→ Reinforces gut-immune connection and role of inflammation (used for background on chronic inflammation).
Note: All remedy instructions, dosages, cautions, and contraindications are pulled directly from these sources. No external studies or fabricated citations are used.

When I Pee It Hurts at the End Female Home Remedy: for Quick Relief
Experiencing pain at the end of urination can be uncomfortable and concerning. For women, this discomfort, often referred to as dysuria, can stem from various causes, including urinary tract infections (UTIs) or irritation. Thankfully, there are several home remedies and lifestyle changes that can help ease this pain. In this article, we’ll explore effective strategies to find relief when i pee it hurts at the end female home remedy, focusing on natural remedies that can provide comfort and support your overall urinary health.
Key Takeaways
- Stay hydrated by drinking plenty of water to dilute urine and flush out irritants.
- Cranberry juice may help prevent bacteria from sticking to the urinary tract.
- Baking soda can neutralize urine acidity, potentially easing discomfort.
- Wearing loose-fitting clothing can reduce irritation in the pelvic area.
- Heat therapy, like warm baths or heating pads, can soothe pain and discomfort.
Understanding Painful Urination Causes
Common Causes of Dysuria
Okay, so dysuria, or painful urination, can stem from a bunch of different things. For women, the most common culprit is a urinary tract infection (UTI). Basically, bacteria sneak into your urinary tract and cause an infection. But it’s not always that simple. Sometimes, the cause isn’t so obvious, and doctors might need to run some tests to figure it out. Other potential causes include:
- Bladder infections (cystitis)
- Vaginal infections
- Inflammation of the urethra (urethritis)
- Sexually transmitted infections (STIs)
It’s important to remember that painful urination can also be caused by irritants like soaps, perfumes, or even kidney stones. If you’re experiencing this, it’s best to get it checked out to rule out anything serious.
Symptoms to Watch For
The main symptom is, well, pain when you pee. But it’s not always the same kind of pain. Some women describe it as a burning sensation, others as stinging or itching. The pain can happen at the start of urination, during, or even right after. If you’re experiencing any of these symptoms, it’s a good idea to pay attention and see if anything else is going on. Here are some other symptoms that might pop up:
- Frequent urge to urinate
- Cloudy or strong-smelling urine
- Pain in your lower abdomen
When to Seek Medical Attention
While some cases of painful urination might clear up on their own with increased fluid intake and home remedies for urinary pain, there are times when you absolutely need to see a doctor. Don’t wait if:
- You have a fever
- You notice blood in your urine
- Your pain is severe or doesn’t improve after a few days
- You have a history of frequent UTIs
These could be signs of a more serious infection or other underlying issue that needs medical treatment. It’s always better to be safe than sorry when it comes to your health. Ignoring these symptoms could lead to complications, so get it checked out!
Hydration and Its Importance

Benefits of Drinking Water
Okay, so, water. We all know we should drink more, but sometimes it’s hard to remember, right? But seriously, when you’re dealing with that
Natural Remedies for Relief
Cranberry Juice Benefits
Cranberry juice is often touted as a go-to remedy, but let’s be real about what it can and can’t do. It contains compounds that can help prevent bacteria from sticking to the walls of the urinary tract. However, it’s more effective as a preventative measure than a cure once an infection has already taken hold. Make sure you’re drinking pure cranberry juice, not the sugary stuff that’s basically juice cocktail.
Baking Soda Solution
Baking soda? Yep, it’s not just for baking. Some people swear by baking soda to neutralize the acidity of urine, which can reduce the burning sensation. Here’s how you might try it:
- Mix 1/2 teaspoon of baking soda in 8 ounces of water.
- Drink it once or twice a day.
- Don’t overdo it, as too much baking soda can mess with your electrolyte balance.
It’s important to note that while some find relief with baking soda, it’s not a substitute for medical treatment, especially if you suspect a UTI. If symptoms persist, consult a healthcare professional.
Aloe Vera Juice
Aloe vera isn’t just for sunburns; it can also be consumed. Some believe that drinking a small amount of pure aloe vera juice can help soothe the urinary tract. It’s thought to have anti-inflammatory properties that might ease discomfort. When looking for natural treatments for female urinary discomfort, aloe vera juice is a good option. However, it’s crucial to use pure aloe vera juice and to start with a small amount to see how your body reacts. Some people experience digestive upset, so proceed with caution.
Lifestyle Changes to Consider

Sometimes, the little things we do every day can make a big difference in our health. When it comes to that uncomfortable feeling when you pee, some simple lifestyle tweaks might offer relief and even help prevent future issues. It’s not always about drastic changes, but more about being mindful of your body and habits.
Wearing Loose Clothing
Tight clothes, especially around the groin area, can trap moisture and create a breeding ground for bacteria. This can lead to irritation and increase the risk of urinary tract infections (UTIs). Opting for loose-fitting clothing, particularly cotton underwear, allows for better airflow and reduces moisture. Think breathable fabrics and comfortable fits. It’s a small change that can make a noticeable difference.
Avoiding Irritants
Certain soaps, douches, and feminine hygiene products contain chemicals that can irritate the urethra and bladder. This irritation can worsen the pain you feel when you urinate. Consider switching to unscented, hypoallergenic products. It might take some trial and error to find what works best for you, but your body will thank you for it. Also, be mindful of scented toilet paper or wipes, as these can also be culprits.
Maintaining Good Hygiene
Good hygiene is always important, but it’s especially crucial when you’re experiencing urinary discomfort. Always wipe from front to back after using the toilet to prevent bacteria from entering the urethra. Also, be sure to wash the genital area gently with mild soap and water daily. Avoid harsh scrubbing, which can cause irritation. Simple, gentle care is often the most effective. Consider probiotics for balance to help maintain a healthy bacterial environment.
Making these lifestyle adjustments can significantly improve your comfort and reduce the frequency of painful urination. It’s about creating a daily routine that supports your urinary health and overall well-being. Remember, consistency is key, and even small changes can add up to big results over time.
Heat Therapy for Discomfort
Heat therapy can be a simple, yet effective way to ease the discomfort associated with painful urination. It works by increasing blood flow to the pelvic area, which can help relax muscles and reduce pain. It’s not a cure, but it can provide temporary relief while you address the underlying cause of your discomfort.
Using Heating Pads
Heating pads are a convenient way to apply heat directly to the affected area. You can use electric heating pads or even microwaveable ones filled with rice or flaxseed. Make sure the heating pad isn’t too hot to avoid burns.
- Always use a cloth barrier between the heating pad and your skin.
- Limit use to 20-minute intervals.
- Avoid falling asleep with a heating pad on.
Warm Baths for Relief
A warm bath can provide overall relief and relaxation. The heat helps to soothe the muscles in your pelvic area, reducing spasms and discomfort. You can add Epsom salts to the bath for added relaxation benefits. Epsom salts contain magnesium, which is known to help relax muscles. If you have the IntimateRose Hot/Cold Pelvic Wand, you can use it in the bath for targeted relief.
- Keep the water warm, not scalding hot.
- Soak for 15-20 minutes.
- Avoid using harsh soaps or bath products that could cause irritation.
Heat Application Techniques
There are several ways to apply heat to your pelvic area. Experiment to find what works best for you. A warm compress is another option. You can make one by soaking a clean cloth in warm water, wringing it out, and applying it to your lower abdomen. Reapply as needed to maintain the warmth. Consistency is key when using heat therapy.
Heat therapy is a great way to manage pain, but it’s important to remember that it’s not a substitute for medical treatment. If your symptoms persist or worsen, it’s important to see a doctor to rule out any underlying medical conditions.
Dietary Adjustments for Prevention
What you eat and drink can really impact your bladder health and how often you experience that “it hurts when I pee” feeling. Making some changes to your diet might help prevent future problems. It’s not a cure-all, but it can be a useful tool in managing your overall health.
Foods to Avoid
Certain foods and drinks are known to irritate the bladder and urinary tract. Cutting back on these might make a difference. It’s not about deprivation, but about being mindful of what you consume. Here’s a quick list:
- Spicy Foods: These can irritate the bladder lining.
- Citrus Fruits: High acidity can cause issues for some.
- Caffeine: Coffee, tea, and soda can increase urgency and frequency.
- Alcohol: Acts as a diuretic and can irritate the bladder.
- Artificial Sweeteners: Some people are sensitive to these.
It’s a good idea to keep a food diary to track what you eat and drink, and note any changes in your symptoms. This can help you identify specific triggers.
Incorporating Probiotics
Probiotics are good bacteria that can help maintain a healthy balance in your gut. Some studies suggest they might also benefit urinary health. You can get probiotics from foods like yogurt, kefir, sauerkraut, and kimchi. You can also take a probiotic supplement, but talk to your doctor first. I’ve found that adding a daily yogurt has helped me feel better overall.
Benefits of a Balanced Diet
A balanced diet is important for overall health, and that includes your urinary system. Make sure you’re getting enough fruits, vegetables, and whole grains. These foods provide essential vitamins, minerals, and fiber. Fiber is especially important for preventing constipation, which can put pressure on the bladder. A healthy diet supports a healthy immune system, which can help prevent infections that lead to painful urination. Consider incorporating diet and exercise into your daily routine for optimal health.
Over-the-Counter Options
Pain Relievers for Dysuria
When you’re dealing with that uncomfortable burning sensation at the end of urination, sometimes you just need quick relief. Over-the-counter (OTC) pain relievers can be a good first step. Medications like acetaminophen or ibuprofen can help reduce the pain and inflammation associated with dysuria. It’s important to follow the dosage instructions on the label and to be aware of any potential side effects. These medications won’t treat the underlying cause, such as a urinary tract infection (UTI), but they can make you more comfortable while you seek further treatment. Remember, if the pain is severe or doesn’t improve after a couple of days, it’s time to see a doctor.
Antacids and Their Use
Believe it or not, antacids can sometimes play a role in managing dysuria symptoms. This is because the acidity of your urine can sometimes irritate the bladder and urinary tract, making the burning sensation worse. Antacids, which are designed to neutralize stomach acid, can also help to reduce the acidity of your urine. This might provide some relief, especially if your dysuria is related to dietary factors or certain medications. Here’s how they can help:
- Neutralize urine acidity.
- Reduce bladder irritation.
- Offer mild symptom relief.
However, it’s important to note that antacids are not a primary treatment for dysuria and should be used in conjunction with other appropriate treatments, especially if an infection is present. If you’re considering using antacids, it’s a good idea to talk to a healthcare professional to make sure it’s safe and appropriate for you.
When to Use OTC Medications
OTC medications can be a helpful tool in managing mild dysuria symptoms, but it’s important to know when they’re appropriate and when it’s time to seek medical attention. Here are some guidelines:
- Mild Symptoms: If you’re experiencing mild burning or discomfort at the end of urination, OTC pain relievers or antacids might provide some relief.
- Short Duration: If your symptoms have only been present for a day or two and aren’t getting worse, OTC medications might be a reasonable first step.
- No Other Symptoms: If you don’t have other symptoms like fever, chills, back pain, or blood in your urine, OTC medications might be sufficient for temporary relief.
However, if you experience any of the following, it’s important to see a doctor right away. Don’t delay seeking medical advice. Phenazopyridine is a medication that can help alleviate pain, but it’s not a cure.
If your symptoms are severe, persistent, or accompanied by other concerning symptoms, it’s important to seek medical attention. OTC medications can mask the symptoms of a more serious underlying condition, such as a UTI or kidney infection, which require prompt treatment with antibiotics. Delaying treatment can lead to complications, so it’s always best to err on the side of caution.
Final Thoughts on Managing Painful Urination
Dealing with pain when you pee can be really uncomfortable and frustrating. It’s important to remember that while home remedies, such as “when i pee it hurts at the end female home remedy,” can help ease the discomfort, they aren’t a substitute for professional medical advice. Drinking plenty of water, avoiding irritants, and using heat therapy are some simple ways to find relief. However, if the pain continues or you notice other symptoms like fever or blood in your urine, don’t hesitate to reach out to a healthcare provider. They can help identify the cause and get you the right treatment. Taking care of your urinary health is key, so listen to your body and seek help when needed.
Frequently Asked Questions
What causes burning pain when I pee?
Burning pain when urinating can happen due to urinary tract infections (UTIs), kidney stones, or irritation from soaps and personal care products.
How can I relieve painful urination at home?
You can drink more water, try cranberry juice, or use baking soda mixed with water to help reduce discomfort.
When should I see a doctor for painful urination?
If the pain lasts more than a day, or if you have fever, blood in your urine, or severe pain, you should see a doctor.
Is it important to stay hydrated?
Yes, drinking enough water helps dilute your urine and can flush out bacteria, reducing irritation.
What lifestyle changes can help prevent painful urination?
Wearing loose clothing, avoiding irritants like caffeine and spicy foods, and practicing good hygiene can help prevent discomfort.
Are there over-the-counter medications for painful urination?
Yes, medications like Uristat® or AZO® can help relieve pain and discomfort associated with urination.


What Is Complex PTSD vs PTSD? The Difference That Changes Everything About Treatment

The World’s Best Longevity Summit (Literally!)

11 Best Teas for Sleep, Ranked by the Research Behind Them

PEMF Webinar

Why You Can’t Trust Big Pharma

The 4-7-8 Breathing Technique: Step-by-Step Guide and What the Research Actually Shows
-
 Events2 weeks ago
Events2 weeks agoPEMF Webinar
-
 Events2 months ago
Events2 months agoWhy You Can’t Trust Big Pharma
-
 Natural Sleep Remedies2 months ago
Natural Sleep Remedies2 months agoThe 4-7-8 Breathing Technique: Step-by-Step Guide and What the Research Actually Shows
-
 Events3 months ago
Events3 months agoBeyond the Brain
-
 Events2 months ago
Events2 months agoThe Anti-Cancer Body with Dr. Michael Karlfeldt
-

 Events4 weeks ago
Events4 weeks agoHBOT ( Hyperbaric Oxygen Therapy ) Webinar
-

 Events1 month ago
Events1 month agoWhole Body Detox Summit
-
 Events1 month ago
Events1 month agoThe Cancer Conversation Your Oncologist Cannot Have in 15 Minutes